Updated: 27 July 2014
Dearly beloved,We are gathered here today because a change is happening, one that we in the transfusion medicine (TM) community should all be aware of, the death of the precautionary principle in transfusion medicine (TM). But life goes on, and now we see the birth of risk-based decision making (RBDM), which is probably at the toddler stage.
Lean and Sigma Six was the flavour of the decade in blood centres and transfusion services. I can only imagine how much money consultants made and still make off this cash cow. Now the new cash motherload for consultants is RBDM.
The blog's title derives from a Pete Seeger classic of the 1950s.
I decided to blog about RBDM because it was featured in the June issue of AABB News in the form of a report on the 2014 National Blood Foundation (NBF) Leadership Forum in Washington, DC on 28 April.
Although AABB News is 'news lite' compared to the full strength journal,Transfusion, I wonder how many working professionals (technologists, nurses, physicians) read the NBF forum report. I suspect few.
But here's the thing. It's worth reading on several levels, including the ability to pass top executives in the hallways of power and quip,
- 'Hey, Graham. How's our transformational innovation going? And do we have any adjacent initiatives on the burner?
- Appropriate Use of Medical Resources, Risk-Based Decision Making and Strategies for Innovation
RBDM - A PARADIGM SHIFT?
RBDM is a major initiative of the The Alliance of Blood Operators (ABO). ABO is international, at least for developed countries. ABO would not make sense for poor countries, which have little or no money to prevent kids dying from diarrhea, let alone effectively prevent risks to the blood supply.
From what I can tell, RBDM is a process for high level leadership dudes to decide things like whether to implement new blood safety measures or not. Its ascendancy signals that the precautionary principle is truly dead. As Thomas Kuhn may have said, there's been a paradigm shift, folks.
Sorry, I know using 'paradigm shift' to describe abandoning the precautionary principle for RBDM is an abuse of what Kuhn meant, but the phrase is one of the most abused ever.
By paradigm, Kuhn meant a 'set of assumptions, definitions, laws and techniques that are shared by the members of a scientific community.' That has since been expanded to relate to members of any community, including the transfusion medicine community and is used in the 2014 paper by Menitove, et al., cited below.
BTW, if you've never read The Structure of Scientific Revolutions, give it a try. It's accessible and fascinating:
By examining history, Kuhn explained why incorrect scientific ideas persist and how they're finally rejected. Because people believe what they know, science is inherently conservative. A current scientific theory ('paradigm') is hard to dislodge and takes much evidence or a powerful single piece of evidence to overturn. When this occurs, Kuhn called it a 'paradigm shift'.
So let's look at RBDM to see if it's a TM paradigm shift.
RBDM takes off
RBDM has been around for a few years but is now gaining steam in NA and all developed nations. For example, in Oct. 2010 a consensus conference was held in Toronto, Canada:
- Leach Bennett J, Blajchman MA, Delage G, Fearon M, Devine D. Proceedings of a consensus conference: Risk-Based Decision Making for Blood Safety. Transfus Med Rev. 2011 Oct;25(4):267-92.
- Menitove JE, Leach Bennett J, Tomasulo P, Katz LM. How safe is safe enough, who decides and how? From a zero-risk paradigm to risk-based decision making. Transfusion. 2014 Mar;54(3 Pt 2):753-7.
The goal is to optimize the safety of the blood supply by enabling the proportional allocation of finite resources to mitigate the most serious risks, recognizing that the elimination of all risk is not possible.Leach Bennett is a lawyer whose earlier jobs at CBS included Executive Director, Legal and Risk Management, and Legal Counsel. (LLB is a Bachelor of Laws, LLM a Master of Laws.) The well respected Leach Bennett is also the Chair of The Alliance of Blood Operators (ABO) RBDM Steering Committee.
SMOKE AND MIRRORS?
How did the supposed 'zero-risk paradigm' in transfusion medicine evolve to a paradigm of risk-based decision making (RBDM)? First, there never was a zero-risk paradigm in TM. The public may have wanted zero-risk but TM professionals knew it was impossible. If anything, what ruled after the HIV/HCV transfusion-related tragedies was a precautionary principle paradigm.
Discussing the nuances of the precautionary principle and the pros and cons of applying it (whatever 'it' means) is beyond the scope of this blog and my competence. To me it always meant
- If there was considerable evidence that a serious risk existed, we should try to prevent it, even if it wasn't proven beyond a shadow of a doubt.
That said, 2 papers on the precautionary principle:
- Alter HJ. Pathogen reduction: a precautionary principle paradigm. Transfus Med Rev 2008 Apr;22(2):97-102.
- Wilson K. A framework for applying the precautionary principle to transfusion safety. Transfus Med Rev. 2011 Jul; 25(3):177-83.
Papers on RBDM suggest the paradigm has changed because the COST of preventing some risks is too expensive. For example the opening sentence of
- Menitove JE, Leach Bennett J, Tomasulo P, Katz LM. How safe is safe enough, who decides and how? From a zero-risk paradigm to risk-based decision making. Transfusion. 2014 Mar;54(3 Pt 2):753-7.
Health care costs have risen to 17.4% of US gross domestic product, and health care economists urge a reversal of this unsustainable trend.Leach Bennett in her presentation to the NBF's 2014 leadership conference, under 'Impetus for Change', references the precautionary principle as the TM response to the 1980s blood tragedies but then states:
- [It's] Clear that pursuit of 'precaution at all costs' is unsustainable
- Blood safety decision-making is increasingly complex: science,ethics, social values, economics, public expectations, context

Instead of cost and effectiveness, many risk assessment models put safety first, i.e., consider the severity of a risk and its probability of happening:

Leach Bennett's NBF presentation is well worth reading because it explains where we are going. The science part ('Risk Intelligence'):
Comprehensive patient outcome and quality data, including hemovigilance, will guide decision-making and help define acceptable risk.The 'Effectiveness and Cost' part:
Reliable information and tools will be readily available to balance risks, costs and benefits in a manner which optimizes donor safety and patient outcomes.The entire RBDM Change Agenda: Source: Judie Leach Bennet's 2014 NFB presentation, Risk-Based Decision Making for Blood Safety

And note what's third on the Change Agenda: Blood operators will take an expanded leadership role in vein-to-vein blood safety. In Canada, that would be our national blood suppliers, CBS and Héma-Québec.
Sounds a wee bit like a unilateral power grab, no? And there's that word innovation again.
GESTALT SWITCH
TM's abandoning the precautionary principle to protect blood safety, and now championing RBDM, is not a true paradigm shift, but could be called a 'gestalt switch'.
OMG, you say, not more jargon! Bear with me. I'm just 'tarting up' the RBDM movement to assess cost vs benefit in blood safety with bafflegab that's an alternative to 'paradigm shift'.
Gestalt is a German concept meaning the whole is greater than the sum of its parts. Gestalt means shape (or form) in English. Gestalt is used in psychology to describe an approach which aims to see something as a whole rather than its individual parts.
A gestalt switch requires an emotional and intellectual switch to think differently. For example, what do you see? A white vase? Or 2 black profiles facing each other? To see one or the other requires us to make a gestalt switch.

That's what our TM 'thought leaders' are doing with RBDM. Because of cost constraints, they've designed a completely different way of conceptualizing risks to blood safety and how to prevent them.
- Zero risk is impossible (something we've long known).
- Safety isn't paramount because it's too expensive. Safety is shades of grey.
- Let's promote the change to RBDM as safety first, because that's what the (somewhat deluded) public wants.
- Moreover, let's associate the cost-saving movement with a sexy name like innovation to make it more palatable. For example:
Judie Leach Bennett, once Director of CBS's 'Legal and Risk Management', now heads the CBS 'Centre for Innovation'.
Title of the AABB News report: Appropriate Use of Medical Resources, Risk-Based Decision Making and Strategies for Innovation.INNOVATION BAFFLEGAB
Another speaker at the NBF leadership conference was Brian Quinn, employed by a company owned by Deloitte Consulting, Chicago.
Quinn highlighted innovation in his closing talk, describing three types:
- Core: existing products
- Adjacent: new business areas adjacent to existing core strengths
- Transformational: inventing products and creating new markets
To read more about this new consulting bafflegab on innovation, see
- Managing your innovation portfolio (Harvard Business Review, May 2012)
BOTTOM LINE
The RBDM movement means we've truly jettisoned the precautionary principle (whose application to TM has been flawed at times) for cost uber alles. It's reality and well foreshadowed.
If RBDM prevailed earlier, it's possible that much of what the TM community did since 1981* to protect the blood supply would never have been done. [*When the CDC's MMWR published a report describing cases of a rare lung infection, Pneumocystis carinii pneumonia, in 5 young, previously healthy, gay men in LA.]
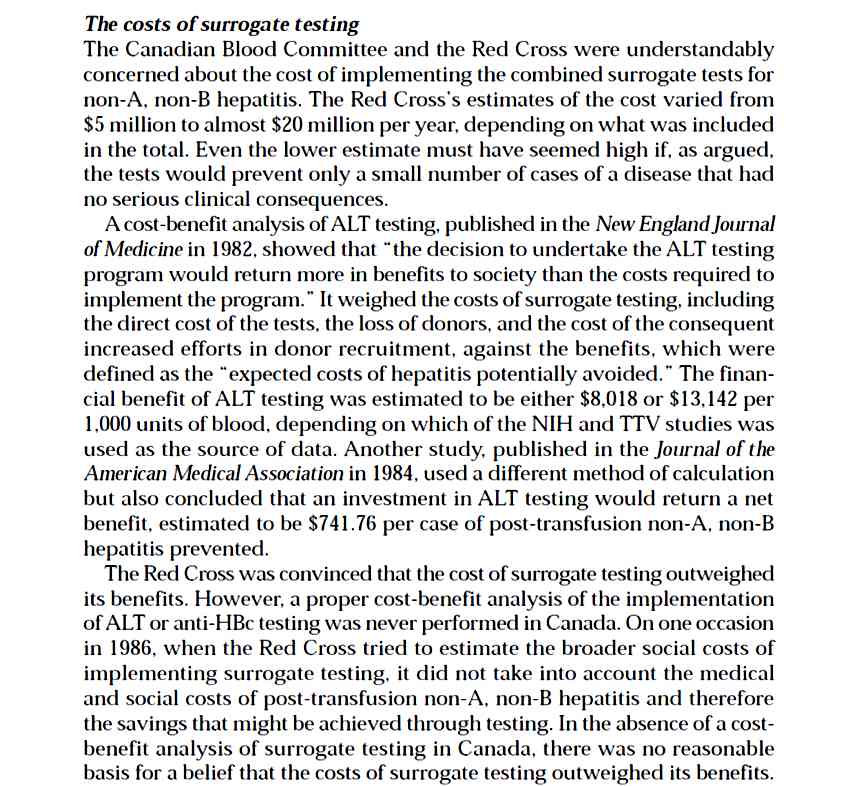
Perhaps a good thing in some cases, but a quasi-cost-effectiveness approach was used decades ago and caused harm, e.g., Canada's decision not to implement surrogate tests for non-A, non-B hepatitis (hepatitis C) because they were too 'unscientific'/ineffective (poor sensitivity and specificity) and too expensive. This decision led to many thousands of Canadians being infected with HCV.
Or the blood supplier (then Canadian Red Cross), clinicians, and government deciding that most hemophiliacs were probably already infected with what became known as HIV, so should continue to receive non-heat treated factor VIII concentrate derived from tens of 1000s of blood donors. Gotta use up that expensive, paid-for stock on the shelves? Seems likely but we'll never know because minutes of crucial meetings were mysteriously shredded.
All of which identifies the flies in the RBDM ointment:
1. TM professionals don't always know what measures are more or less effective to enhance blood safety. Sometimes measures that seem costly at the time and are deemed flawed (ineffective) can save the health care system mega-bucks in the long run, to say nothing of human suffering, as in Canada's hepatitis C debacle.To everything there is a season. The old blood safety season (new season):
2. Just like the public in general, health professionals sometimes get caught up in mob psychology. If thought leaders religiously proselytise a particular policy, it's hard for acolytes to dissent and be designated heretics. Definitely not a good career move.
- 'Above all, do no harm' (Only do no harm if it's cheap and effective.) Note: Doing harm can result from acts of omission.
- 'If harm is suggested, but not proven beyond a shadow of a doubt, we should try to prevent it.' (If harm is possible, don't prevent it unless the measure is cheap and effective.)
- Soon we will spend money only on cheap, effective blood safety measures. All else is no or maybe.
But it's human nature to go for the simplest tool and, because economics fits the bill and is a driver for RBDM, it will likely carry more weight.
In reply to Roger (see comment below): Invariably those making decisions promote safety above all but, when you examine what they say, often a different picture emerges.
Note the words used to soothe the public that all is well, you can trust us. For example:
1) The goal is to optimize the safety of the blood supply by enabling the proportional allocation of finite resources to mitigate the most serious risks, recognizing that the elimination of all risk is not possible.
means, 'We'll spend $ only on the MOST SERIOUS RISKS and only if it's INEXPENSIVE because there's not enough $ to go around.' The other points are background noise to obfuscate the main point.Key words to soothe the public: optimize, safety
2) Comprehensive patient outcome and quality data, including hemovigilance, will guide decision-making and help define acceptable risk.
means, 'We don't have a clue how to decide what acceptable risk is, but, trust us, because we'll use comprehensive, quality data and muddle our way through.'Key words to soothe the public: comprehensive, quality, acceptable
3) Reliable information and tools will be readily available to balance risks, costs and benefits in a manner which optimizes donor safety and patient outcomes.
means, 'You can trust us to decide what's safe. 'Key words to soothe the public: reliable, readily, balance, optimize, safety
The soothing words didn't appear by accident but were carefully crafted. They're not quite weasel words to mislead readers into thinking that a meaningful, specific statement was made. But they do aim to mislead in that they're designed to create the overwhelming impression that RBDM leaders are on top of things, have all bases covered, and put safety first, not saving money.
They make the case that, by not spending money on ineffective, costly measures, blood safety will be enhanced. Hard to argue against that, assuming we know ahead of time what's ineffective (we didn't with surrogate tests for HCV). The rest is sheer 'trust us' territory and, if past is prologue, why would we?
Update #1 (17 July 2014)
In reply to Anonymous who wrote on the reality of scarce resources (see Comments below):
I agree the health care system must prioritize as funds are finite. That's a given. But you set up a false hypothetical in that everyone can agree not to fund your example.
It's the heavy emphasis on costly (cost is easy to determine) prevention measures where things can go awry, especially as history shows experts don't always know what's effective, or even true prevalence, witness HCV when it was non-A, non-B hepatitis.
In Canada, governments have long tried to curb the cost of transfusions, particularly plasma derivatives like IV immune globulin, which have many off-label uses, e.g., the BC PBCO's utilization management program.
Then there's looking at larger priorities for tax dollars in terms of $ spent on the Afghan war, fighter jets we don't even have yet, Canada's Senate, and on and on.
How to spend health resources effectively and fairly is challenging. That's why our TM experts should be challenged on their plans, especially when they choose to wrap it in quasi-weasel-language like transformational innovation.
Update #2 (17 July 2014)
In reply to Anonymous, who wrote, 'We seem to be getting arrogant again in thinking the science alone can manage risk':
My gut reaction is to quip, 'Getting arrogant again? Nope. We never stopped being arrogant.' But you make a point worth discussing.
Today's health professionals, including TM experts, stress evidence-based medicine (EBM), most recently CBS CEO Graham Sher on the issue of paid plasma collection in Canada:
- Purchased plasma safe, essential (8 May 2014)
We have created a safe and secure system that today is the envy of much of the world, and we did this using science, evidence and risk-based decision making as our core principles. It is important that these principles continue to be the driving force behind public policy and the blood system.But EBM is not without its flaws, as explained in this 2011 Boston Globe op ed:
As the author notes, “Evidence-based medicine is only as strong as the evidence used to support it. The stark reality is that evidence can be weak, biased, or even fraudulent.” Amen.
For a comprehensive, straightforward, balanced look at the issues facing blood safety, one not into the current group-speak lingo propagated in many of the other cited papers, see:
- Aprili G. Safety in transfusion medicine. Blood Transfus 2008 Jul; 6(3): 121–6.
In reply Anonymous (x2), about latest news on Ontario's plan to ban paid plasma clinics in Canada:
Intriguing part is ON Dept of Health inspectors 'swooped in to seize records'. Those operating Canadian Plasma Resources clinics said the raid virtually halted operations.
Why a raid to seize records? Can't wait for more details. Stay tuned.
Updated 27 July 2014
In response to the Comment below about two quotes by CBS CEO Graham Sher, I've decided to write a new, separate blog. This one is getting a bit long.
FOR FUN
The theme made me think of Pete Seeger's Turn! Turn! Turn! The lyrics and final verse are adapted word-for-word from Chapter 3 of the Book of Ecclesiastes:
- Turn! Turn! Turn! (Judy Collins)
- Turn! Turn! Turn! (Pete Seeger, 2012)
To everything, turn, turn, turn.As always, the opinions are mine alone and feedback is most welcome.
There is a season, turn, turn, turn.
And a time to every purpose under heaven.
A time to be born, a time to die.
A time to plant, a time to reap.
A time to kill, a time to heal.
A time to laugh, a time to weep.


{kind=link}
{kind=link}