THE PAPER
As it happens there is a recent publication involving economics and transfusion medicine (TM):
- Custer B, Hoch JS. Cost-effectiveness analysis: what it really means for transfusion medicine decision making. Transfus Med Rev 2009 Jan;23(1):112. (PDF, free full text)
Brian Custer, lead author, is with the Blood Systems Research Institute.-->This blog examines the issue of cost effectiveness analysis and its role in influencing blood safety policies. As always, ideas are presented as food for thought.
The authors discuss cost-effectiveness analysis (CEA) in TM, with a focus on blood safety and infectious diseases. For example:
- CEA can help policy makers decide whether or not to implement a test such as HIV-1 p24 antigen (as was done in 1996 but was discontinued ~2003 after HIV NAT testing was licensed).
- CEA can also provide a framework for comparing HBV NAT testing with pathogen inactivation of blood components.
"Blood safety may be different, but the economic concept of efficiency does apply. It is better to pay $10,000,000 to save 1,000 people than to pay 10 times that amount to save 1 person, and it is surely better to reach this decision after looking at the costs and the benefits rather than before."
With economics, like statistics, many people’s eyes glaze over. But read on – it’s fascinating stuff. Below are but a few of the paper's key points.
ECONOMIC CONCEPTS
Economics is about the efficient use of scarce resources and a CEA is one tool that can help decision makers decide which new blood safety test or process to implement.
CEA involves 3 key concepts:
- Since there are insufficient resources to support all possible activities, we must make choices.
- We must decide whether or not to adopt a given intervention and how to allocate resources between competing alternatives.
- In choosing, we must factor in the "opportunity cost", i.e., the value of forgone benefits. In other words, the true cost of something ("A") is not just what "A" costs but also the value of what we did without (the lost opportunity, "B") because we chose "A".
CEAs range from narrow (impact on the budget) to broad (factoring in the cost of human life and the quality of life). The latter analysis is termed cost utility analysis (CUA). CUA results are often given as a ratio of cost to health benefits and are reported as cost per quality-adjusted life year (QALY).
The cost per QUALY is a tool that allows for comparisons of health benefits across diseases. The value of what is considered a cost- effective QALY varies greatly between developed and undeveloped countries, as well as among disciplines.
In general, a cost-effective QALY is considered to be
- Clinical medicine: $50,000 to $100,000/QALY
- WHO: up to 3 times the GDP per person = ~$94,000 in USA & Canada and $72,000 in Europe (in year 2000 $)
Larger QALY ratios are accepted in some areas such as blood safety because of several factors:
- First, do no harm implies a high priority to prevent outcomes such as diseases caused by contaminated blood.
- Society places a relatively high value on preventing low-probability risks with serious consequences.
- Society is willing to support interventions that target identifiable individuals e.g., blood recipients.
For example:
- Anti-HIV screening when first adopted: $3600/QALY (due to higher HIV prevalence in donors & limited use of donor selection strategies)
- HIV p24 antigen testing (since abandoned): $2.0 million/QALY
- HIV NAT: $2.0 million/QALY (even using a NAT minipool, multiplex format with HCV and even with HBV too)
- HCV NAT: >$1.8 million/QALY (minipool)
- WNV NAT: $500,000/QALY (2003 - highest outbreak year)
- HBV NAT: additional $1 million/QALY or more (in multiplex format with HIV and HCV)
- HBV NAT: $66 million/QALY (separate test without HIV and HCV)
- Mechanical barriers to prevent misidentification errors leading to transfusing the wrong ABO group: $197,000/QALY
The following ideas are not particularly profound or original but seem worth stating.
1. Statistics can be used to prove anything.
If you want to inspire confidence, give plenty of statistics. It does not matter that they should be accurate, or even intelligible, as long as there is enough of them.Don’t get me wrong, I love statistics. However, as we know, CEAs and their sub-type CUA generate many statistics and, depending on the assumptions chosen, can be used to justify just about anything.
- Lewis Carroll, mathematician, clergyman, author (1832 – 1898)
This is especially true when decisions involve costs or benefits whose price is unclear or varies, which limits the generalizability of many studies. For example, consider this paper and its assumptions:
AuBuchon JP, Littenberg B. A cost-effectiveness analysis of the use of a mechanical barrier system to reduce the risk of mistransfusion. Transfusion. 1996 Mar;36(3):222-6.Note that costs could change dramatically if the study's few assumptions changed. As a result economic studies have to be assessed carefully and taken with a huge block of salt.
Unfortunately, critical assessment of economic papers is often beyond the grasp many health practitioners.
- Whenever statistics are tossed about, the potential for Taurus excreta cerebrum vincit exists. (Latin is incorrect, but you get the idea.)
Undoubtedly, the history of the "tainted blood" scandals of the 1980s and 1990s involving HIV and HCV have influenced society's willingness to accept interventions that are not cost effective when compared with other areas of medicine. As has been noted so often by the TM community, citizens have come away from the HIV/AIDS tragedy with the impossible desire for a zero-risk blood supply.
Regrettably, in attempting to achieve zero risk, with tests for infectious diseases with common risk factors, we run into the law of diminishing returns. Because each test or intervention is layered upon previous ones, we inevitably spend more and more to detect fewer and fewer infections until the "bang for the buck" is minimal and the QALY cost is prohibitive.
3. Legal concerns
The threat of legal action remains influential in TM policy decisions, as in all of health care, and contributes to higher costs. As quoted by Custer and Hoch, regarding the decision to implement leukoreduction in Belgium:
The core problem proved to be legal. The blood banks are legally accountable for blood safety. This accountability is absolute, based on avoidance of all possible risks, regardless of costs. This strategy leads to inefficiencies in health care (i) blood safety management is guided by available rather than cost-effective technology, and (ii) private insurance premiums for civil liability are sharply increasing, while they are in no way related to the expected returns and the high and increasing [cost of] blood safety.Source: Cleemput I, Leys M, Ramaekers D, et al: Balancing evidence and public opinion in health technology assessments: The case of leukoreduction. Int J Technol Assess Health Care 22: 403-407, 2006.
Government settlements to victims of transfusion-related diseases have been substantial, for example:
- Irish Hep C payout tops €818m
- Japan payout over tainted blood
- Angelotta C, McKoy JM, Fisher MJ, Buffie CG, Barfi K, Ramsey G, et al. Legal, financial, and public health consequences of transfusion-transmitted hepatitis C virus in persons with haemophilia. Vox Sang 2007 Aug;93(2):159–65.
4. CUA versus the precautionary principle
Cost utility analysis (CUA) is about allocating resources between competing alternatives. CUA calculates a ratio of cost to health benefits that is reported as cost per quality-adjusted life year or QALY.
Custer and Hoch write:
- It is better to pay $10,000,000 to save 1,000 people than to pay 10 times that amount to save 1 person….
Unfortunately, real world choices are almost always much messier. Then there is the precautionary principle, which was extensively reviewed in an earlier blog:
This CMAJ commentary (The Krever Commission – 10 years later) discusses Canada’s approach to the precautionary principle:
- The tainted blood tragedy was arguably the worst public health catastrophe in Canada's history.
- Guided by the Krever Commission findings, Canada's reformed blood system has restored public confidence in blood safety by proactively addressing infectious risks.
- Two influential concepts from the Krever Commission have contributed to the reformed blood system's success: the adoption of precautionary measures and the creation of a governance system with clearer roles and responsibilities, including the separation of funding from decision-making concerning safety.
The adoption of the precautionary approach has partly contributed to a mentality that is highly averse to risk that has led to the introduction of some safety measures considered to be cost-ineffective, with costs per quality-adjusted life-years sometimes in the millions…. Now that Canada has distanced itself from the tainted blood tragedy, and that public confidence in the blood system has been re-established, officials have the luxury of re-examining safety priorities and the correct balance between safety and cost.I interpret the author as saying that we in Canada went overboard with the precautionary principle - now let’s get with the correct balance, whatever that is.
5. History as prologue
I cannot help but recall a few quotations about history:
- Those who cannot learn from history are doomed to repeat it. (George Santayana)
- History repeats itself, first as tragedy, second as farce. (Karl Marx)
- The charm of history and its enigmatic lesson consist in the fact that, from age to age, nothing changes and yet everything is completely different. (Aldous Huxley)
- History will be kind to me for I intend to write it. (Winston Churchill)
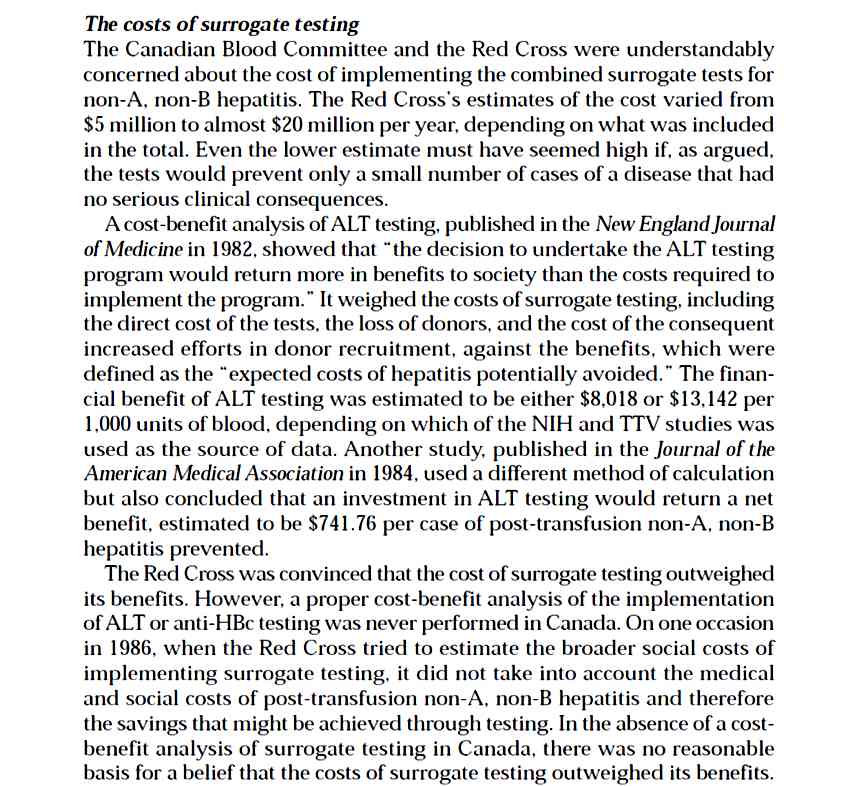
From 1986 to 1990 Canada, like many other countries, did not implement surrogate tests for what was then called non-A, non-B hepatitis. If an extensive CEA had been done of surrogate tests, the results would probably have been that the tests (anti-HBc and ALT screening) were not cost-effective. Regardless of the sensitivity and specificity of both screens (poor), the CEA's key assumptions would likely have been wrong. They would have underestimated the extent of the disease and its eventual health consequences. Regardless, such a CEA was not done.
- See this excerpt from the Krever Report (p. 695)
BOTTOM LINES
1. GIGO. One of the main challenges with CEA and CUA is, as the computer nerds say, GIGO, Garbage in, garbage out or more likely where computer-generated statistics are concerned, Garbage in, Gospel out.
2. QALY. Statistical gobbledegook involving numbers, poorly understood concepts, and loads of money can baffle even the most astute among us. Fess up – do you really understand QALY?
“The idea of QALY is to put a value on treatments that may not save lives but improve them. For example, if a blind person’s quality of life is “worth” 0.75 points per year, a treatment that would restore him to perfect vision — and raise his quality of life to 1 per year — is worth 0.25 per year of life. If the person lived another 30 years, the treatment would be worth 7.5 QALYs, or 30 times 0.25.”
Source: Berenson A. Pinning down the value of a person’s life (see Further Reading)Say what? QALY, schmally, this type of creative number crunching is perverse even without all the iffy assumptions that go into producing the final numbers.
3. Dr. Strangeblood. Perhaps it’s because the transfusion-associated AIDS tragedy seems very recent to me, but whenever people start to promote cost effectiveness studies for blood safety measures, I get nervous.
Judicious use of public money is only common sense given that the money pot is finite. But, inevitably, when suits with calculators take control, even Dr. Strangebloods in suits with stethoscopes around their necks, humanity seems to fade.
People become numbers, money becomes paramount, and medicine becomes just another business. Is that what will protect the blood supply from another HIV tragedy?
Maybe I’m just a bleeding heart but I’m starting to worry and hate the numbers. I cannot get around the concern for love nor money. Take your pick:
ADDENDUM: Statistical tidbits (see paper's references for sources):
Infectious disease risks (USA)
HIV:1 per 2.3 million donations
HCV: 1 per 1.8 million donations
HBV: between 1 per 63,000 to 205,000
Non-infectious risks (examples of interventions)FURTHER READING
TRALI from plasma:1 per 100,000 (male-only plasma)
Fatal septic transfusion reaction from platelets: 1 per 140,000 (mandatory testing)
Major mismatch of ABO type:1 per 600,000 (mechanical barriers, bar coding, RFID)
Government of Canada. Hepatitis C - Compensation for Tainted Blood Victims
Krever H. The blood supply system in Canada: systemic problems in the 1980s. Commission of Inquiry on the Blood System in Canada. Final report. Ottawa: Canadian Government Publishing; 1997;989.
(click "continue to the document")Hill B. Zero risk at all cost in blood transfusion. Biomed Scientist, April 2005. (PDF)
Krever - Vol. 1: The background
Krever - Vol. 2: Where much of the "nitty-gritty" controversy is investigated and discussed
Of particular interest and relevance:
#24 - Canada's rejection of surrogate testing
Krever - Vol. 3 - International responses to the risk of HIV in the blood supply
Berenson A. Pinning down the value of a person’s life. New York Times, June 11, 2007.
Staginnus U. Health economics research on blood transfusion safety measures - an introductory primer. In Peterson BR.ed. New Development in blood transfusion research. Nova Science Publishers, 2006.
Comments are most welcome BUT, due to excessive spam, please e-mail me personally or use the address in the newsletter notice.

{kind=link}