Updated: 4 Jan. 2020 (Updated song's link)
Apparently being thankful can improve your life. A professor of psychology at the University of California says so. It must be true (she wrote with tongue in cheek). Actually (and I hate writing or saying 'actually' after hearing a news reporter begin every sentence with it), I suspect it's true in most circumstances. Not necessarily when linked to being obsequious, though.
I had earlier written another blog for October on a topic I often blog about (two guesses - see below) but rethought it, especially since it's Canada's Thanksgiving today. Accordingly, this month's blog is about three things I feel thankful about it in the world of transfusion medicine and two that I don't.
Despite the Canadian references, transfusion professionals worldwide should be able to relate. As you read, I encourage you to think about your career and assess if any of my musings agree with yours. Please feel free to comment.
The blog's title derives from 1970 Simon and Garfunkel classic, one of my favorites.
TOP THREE 'THANKFULS'
#1. Career in Transfusion Medicine
My life in TM began by accident and I never should have been hired. I was a high school teacher who wanted to work in Winnipeg but jobs were hard to come by for a 21 year old with a year's experience teaching in a rural Manitoba 4-room high school.
Lo and behold - a friend said, 'Pat, Canadian Red Cross Blood Transfusion Service hires BSc grads because most med lab tech grads from Red River Community College are scared to work there.' Say, what? I later learned the fear was largely because the clinical rotation was pathetic. Students spending most time labelling tubes and similar scut work in between being told by technologists to get the ABO group right or they could kill a patient. Did I mention the clinical rotation was only 2 weeks then?
Soon I started work in a large combined blood centre and transfusion lab, the latter doing compatibility testing for all city hospitals and beyond, plus prenatal testing for northwestern Ontario. At first, I did not even know what the yellow stuff was when the red cells settled. True story. Could never happen today, a good thing.
I'm so thankful for the mentoring of generous colleagues. And for wanting and needing to read the 'bibles' of TM from front to back (every word). The books were penned by such icons as Issitt and Mollison, and included the AABB Technical Manual and a 'little red book' written for Red Cross staff by Dr. B.P.L. (Paddy) Moore (and others), National Director of the Red Cross Blood Group Reference Laboratory, who died in 2011. I wrote about Dr. Moore in a 2007 blog, 'My life as a blood eater.'
I worked in Winnipeg for 13 years, got Subject certification in Transfusion Science (no longer offered) from what is now CSMLS. My last 3 years were as the clinical instructor for new laboratory staff, RRCC students, and medical residents doing a transfusion medicine rotation in the only show in town. How crazy is that?
Looking back, I'm thankful that I worked in a busy laboratory where you never knew what to expect. Besides the routine of pretransfusion testing for scheduled surgery and anemic patients, at any time 24/7 patients might need massive amounts of blood in a hurry from a ruptured aneurysm to a GI bleed to a placenta previa during delivery. Often the lab was chaotic but it was organized chaos, even if that's an oxymoron.
Moreover, I'm thankful that in those days work was mostly hands-on and issues arose daily that required problem solving. For example, I worked with Dr. John Bowman when he did the first trials of antenatal Rh immune globulin and was involved in the work that led to this paper (I'm the Pat mentioned in the paper):
- Lewis M, Kaita H, Anderson C, Chown B. Independence of Colton blood group. Transfusion. 1971 Jul-Aug;11(4):223-4.
For an absolute hoot, when you have some time for 'mindfulness' reading, see these articles from 45 years ago by Canadian Red Cross staff, including Dr. B.P.L. Moore. The second includes, 'The possible future role of automated tests on blood donations is briefly discussed.' (Emphasis is mine.)As to my career, the rest is history.... I'm thankful that I lucked out getting a teaching job in Medical Laboratory Science, University of Alberta, where I had the privilege of again working with generous, talented colleagues and teaching 100s of bright, inquisitive students, who kept me on my toes and forced me to keep learning. To be honest, at MLS I believe I had the best job teaching blood bank in the entire world.
- Moore BP. Automation in the blood transfusion laboratory: I. Antibody detection and quantitation in the technicon autoanalyzer. Can Med Assoc J. 1969 Feb 22;100(8):381-7.
- Meade D, Stewart J, Moore BP. Automation in the blood transfusion laboratory. II. ABO grouping, Rh and Kell typing, antibody screening, and VD testing of blood donations in the autoanalyzer. Can Med Assoc J. 1969 Nov 1;101(9):35-9.
Thinking about a career, particularly in later years, makes you realize how lucky you have been. I'm thankful to have worked in the trenches of blood banking doing work that made a difference and then to have gotten a job where that knowledge and skill could be passed to others. I hope that's true for you too.
As an aside, I'm thankful that I learned how to create web sites before it was easy (and you needed to know html code), which has stood me in good stead over the years, especially after I left real work.
#2. Living in Canada
The good points of living in Canada are obvious, but that's not where I want to go. I imagine residents of many countries feel privileged for various reasons.
Instead, in keeping with the transfusion theme, I'm thankful that today Canadians are free to criticize CBS and our blood system leaders. Goodness knows, I do plenty of that and live to write another day.
October's TraQ newsletter has examples of criticism and responses to it:
- CBS tells staff that national blood inventory levels are at their lowest since 2008. In a Sept. 30 memo, Chief Supply Chain Officer Ian Mumford calls it a 'serious performance gap.' (Source: OPSEU blog, 6 Oct. 2014)
- CBS leadership should resign after admitting failure, says Ontario Public Service Employees Union president (OPSEU represents most CBS employees in Ontario)
- CBS apologizes for referring to homosexual sex as a 'behaviour.'
- Fascinating interview with Dr. Mark Bigham, Medical Officer, CBS Vancouver.
- Full credit to Dr. Bigham for doing what must have been an awkward interview and not defensively arguing, as he could have, about what a 'behaviour' is or is not.
In many countries criticism of perceived authority is not allowed. And in some democracies health care workplaces exist where questioning prevailing orthodoxy, especially by those lower in the pecking order, is discouraged, even risky, career-wise. I'm grateful that's not true in Canada's transfusion medicine community, at least not the one I've been fortunate to work in.
Interesting that PPTA's Fall 2014 issue of The Source includes David Page's article, as well as an article by CBS CEO Graham Sher:
Dr Sher's take home message is the same as he's espoused in Canada;
#3. UK's SHOT
The UK's haemovigilance scheme (why is everything in UK TM a 'scheme'?), known universally as SHOT (Serious Hazards of Transfusion), is a world leader in hemovigilance.
The prior blog discussed an example from the 2013 SHOT report on how errors occur and touted it as a great CE resource.
The UK's haemovigilance scheme (why is everything in UK TM a 'scheme'?), known universally as SHOT (Serious Hazards of Transfusion), is a world leader in hemovigilance.
Note, I've dropped the 'ae' diphthong, which still rears its ugly head in Canada, a carryover from transplanted Brits running our blood system. (big grin).I'm thankful for SHOT, a godsend to TM professionals globally and one of the best tools for education and quality improvement ever. As an educator, I use it repeatedly to make instruction real to students and professionals alike.
The prior blog discussed an example from the 2013 SHOT report on how errors occur and touted it as a great CE resource.
- Stand by me (Musings on effects of errors on transfusion professionals)
I've mentioned SHOT again in order to emphasize one of the 'Bottom Two' issues below that I'm NOT thankful for.
One of the best parts of SHOT's reports are its case studies, which detail exactly what went wrong and provide learning points. As but one example from SHOT 2013:
TWO NOT-THANKFULS
To give the blog a dash of hard cold reality and move from 'Kumbaya' territory, two TM realities I'm not grateful for:
NOT Thankful For #1
Canada's lack of a hemovigilance reporting similar to SHOT, where TM practitioners and educators alike, can see how our TM system is doing. Oh wait! Instead of the usual archived SILENCE, all of a sudden, TTISS is online with - wait for it - summary tables:
For interest, I blogged about Canada's lack of hemovigilance reporting in 2011:
Health Canada's stonewalling on Ontario's paid plasma clinics. I've blogged about this many times. HC's public consultation from April 2013 has transmogrified into SILENCE as 2015 approaches. Hmmm...
The one thing perhaps to be grateful for is the hope that 'no news is good news.' Not holding my breath.
LEARNING POINTS
1. I hope all readers can say they love their careers as I love mine. In some ways the 20th C was a golden age, especially for those of us who love immunohematology.
Work is something we do, first to provide essentials like shelter and food, second to be able to appreciate the good things in life that aren't free, and third, to make a difference in the world - to make life better for each other.
TM professionals are truly fortunate to love going to work each day and to be able to question authority. For so many on the planet that's not true. Best of all is knowing we make a difference, each in our small way. It's captured by Mary Oliver in her poem, The Summer Day:
3. Some national blood systems spend time, energy, and money on improving transfusion practice and generously share it with the rest of us. The best example is SHOT, funded by the UK Blood Services. Kudos to NHSBT. Wish Canada and the USA would do more of the same. Hope springs eternal...
FOR FUN
Why? Mainly because I'm grateful for this song and appreciate its lyrics.
Also, because one of the best things in life is to be grateful for our friends.
Added 25 Nov. 2014
In reply to Anonymous, who notes Globe and Mail article:
Seems CPR will try to open paid plasma collection centres in western Canada, likely BC or Alberta [vs Saskatchewan or Manitoba, where a paid plasma clinic exists in Winnipeg, but for plasma containing special antibodies, e.g., anti-D to produce Rh immune globulin)] because of their larger populations and openness to private medical facilities.
About CPR collecting plasma for research purposes in Ontario, I agree it would be interesting to see the protocol and informed consent for such a proposal. Thanks for the comments.
Added 3 Nov. 2014
In reply to Anonymous, who writes about introducing paid plasma clinics in Ontario:
The link provided by Anonymous is to a paper in the Fall 2014 issue of The Source, a PPTA publication:
One of the best parts of SHOT's reports are its case studies, which detail exactly what went wrong and provide learning points. As but one example from SHOT 2013:
- Case 3: ABO incompatible transfusion despite a robust system of warning alerts on the laboratory information management system (LIMS)
- Search for 'Case 3' (without the quotation marks)
" An ABO incompatible red cell unit was transfused resulting in a haemolytic transfusion reaction. The blood was issued using an emergency protocol on the LIMS, which was not appropriate for the non-urgent clinical situation, and the computer warning flag stating that the units were incompatible was overridden several times by the biomedical scientist (BMS).Good stuff, no?
This incompatibility was not noted at the bedside and when the patient reacted to the transfusion, the doctor who was consulted advised that the transfusion should continue without reviewing the patient. The patient developed acute and delayed haemolysis, but no long-term sequelae."
TWO NOT-THANKFULS
To give the blog a dash of hard cold reality and move from 'Kumbaya' territory, two TM realities I'm not grateful for:
NOT Thankful For #1
Canada's lack of a hemovigilance reporting similar to SHOT, where TM practitioners and educators alike, can see how our TM system is doing. Oh wait! Instead of the usual archived SILENCE, all of a sudden, TTISS is online with - wait for it - summary tables:
- Transfusion Transmitted Injuries Surveillance System (TTISS) Summary Results for 2006 - 2012
For interest, I blogged about Canada's lack of hemovigilance reporting in 2011:
- Only in the UK and 'Down Under'? Pity! (Musings on hemovigilance)
Health Canada's stonewalling on Ontario's paid plasma clinics. I've blogged about this many times. HC's public consultation from April 2013 has transmogrified into SILENCE as 2015 approaches. Hmmm...
The one thing perhaps to be grateful for is the hope that 'no news is good news.' Not holding my breath.
LEARNING POINTS
1. I hope all readers can say they love their careers as I love mine. In some ways the 20th C was a golden age, especially for those of us who love immunohematology.
Work is something we do, first to provide essentials like shelter and food, second to be able to appreciate the good things in life that aren't free, and third, to make a difference in the world - to make life better for each other.
TM professionals are truly fortunate to love going to work each day and to be able to question authority. For so many on the planet that's not true. Best of all is knowing we make a difference, each in our small way. It's captured by Mary Oliver in her poem, The Summer Day:
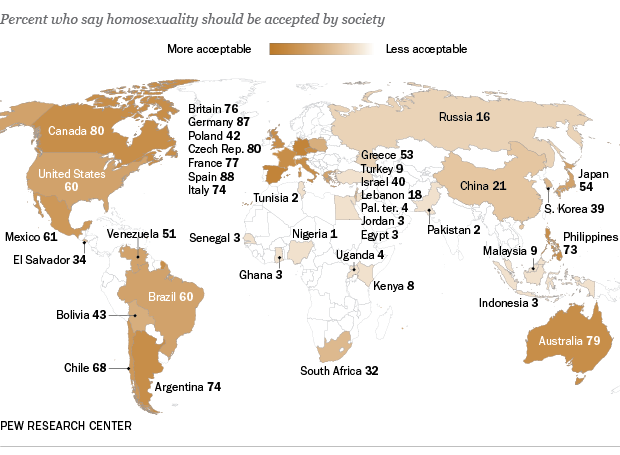
2. Where we live is an accident of birth. We in the industrialized west are so fortunate. Search Google's images for 'children garbage dumps' for 1000s of examples. Or people who say homosexuality should be accepted or places where female genital mutilation commonly occurs.'Tell me, what is it you plan to dowith your one wild and precious life?'
3. Some national blood systems spend time, energy, and money on improving transfusion practice and generously share it with the rest of us. The best example is SHOT, funded by the UK Blood Services. Kudos to NHSBT. Wish Canada and the USA would do more of the same. Hope springs eternal...
FOR FUN
What was my original Oct. blog's topic? Two guesses (my favorite 'hobby horses'):Now, on to the fun music selections. On the two TM issues I'm NOT grateful for, the song that comes to mind is Simon and Garfunkel's 1964 classic, 'The Sound of Silence,' #156 on Rolling Stone's list of the 500 Greatest Songs of All Time and one of the most covered songs of the 20th C.
A. Paid plasma clinics
B. HIV/AIDS
For clue, look at TraQ's Oct. newsletter.
- The Sound of Silence (Simon and Garfunkel, Live in Central Park, 1981)
Why? Mainly because I'm grateful for this song and appreciate its lyrics.
Also, because one of the best things in life is to be grateful for our friends.
- Bridge Over Troubled Water (Simon and Garfunkel, Live in Central Park, 1981)
When you're weary, feeling small,As always the views are mine alone and comments are most welcome. Does any of this ring true? What are you grateful for these days?
When tears are in your eyes, I will dry them all.
I'm on your side. When times get rough
And friends just can't be found,
Like a bridge over troubled water
I will lay me down.
Added 25 Nov. 2014
In reply to Anonymous, who notes Globe and Mail article:
- Canadian Plasma Resources gives up on plan to open plasma clinics in Ontario (24 Nov. 2014) and comments
- "I don't understand how they could pull out but still hope to continue drawing plasma for research purposes. It would be interesting to see the protocol and Informed Consent on this proposal."
Seems CPR will try to open paid plasma collection centres in western Canada, likely BC or Alberta [vs Saskatchewan or Manitoba, where a paid plasma clinic exists in Winnipeg, but for plasma containing special antibodies, e.g., anti-D to produce Rh immune globulin)] because of their larger populations and openness to private medical facilities.
About CPR collecting plasma for research purposes in Ontario, I agree it would be interesting to see the protocol and informed consent for such a proposal. Thanks for the comments.
Added 3 Nov. 2014
In reply to Anonymous, who writes about introducing paid plasma clinics in Ontario:
- "Policy decisions of this nature should not be made without hearing from those who are affected the most by the legislation: that is, the recipients of plasma-derived medicinal products represented by their associations”:
The link provided by Anonymous is to a paper in the Fall 2014 issue of The Source, a PPTA publication:
- 'Compensation for Plasma Donation in Ontario: A Cautionary Tale' by David Page, National Executive Director of the Canadian Hemophilia Society
Interesting that PPTA's Fall 2014 issue of The Source includes David Page's article, as well as an article by CBS CEO Graham Sher:
Dr Sher's take home message is the same as he's espoused in Canada;
- [Paid plasma] is an issue of public policy, not product or patient safety.
- Pharmaceuticals made with plasma from paid donors are safe, lifesaving products for patients in Canada and around the world.
- Canadian Blood Services remains committed to voluntary donation for its donors.
Sher's article is PRO PAID PLASMA (my interpretation): Because paid plasma is safe, to use it or not depends on government policy.Without paid plasma, people would die. But, hey, CBS is committed to a voluntary blood system.
The PPTA would not publish articles that were anything but PRO PAID PLASMA.
Further Reading
- The Source, Fall 2014 (Industry publication)
- The twisted business of paid plasma (The Atlantic, May 2014)
- Earlier blogs on paid plasma (Search at top left for 'paid plasma')

{kind=link}
{kind=link}
{kind=link}